HHS report falsely claims higher drug spending is driven by higher drug prices
The Biden administration recently released two reports to “illustrate the positive impact of the Inflation Reduction Act on prescription drug prices.” That’s how the headline of the Department of Health and Human Services (HHS) press release described the lesson to draw from the two reports.
However, a close review of the reports shows they don’t support key claims in the press release. In fact, the leading claim from one report appears to state the exact opposite from what the data in the report shows. Specifically, the press release and the report claim, as the press release states, “Spending growth on drugs was largely due to growth in spending per prescription, and to a lesser extent by increased utilization (i.e., more prescriptions).” Yet, the data in the report show that it’s utilization, not pricing, that’s the primary driver of higher prescription drug spending.
Blaming drug prices key to justifying IRA
Among all the claims in the two reports, this is the most important claim to support the Inflation Reduction Act (IRA). If the price per prescription drug is indeed the primary driver of higher prescription drug spending, then the IRA’s focus on lowering prescription drug prices makes some sense. And it supports ASPE’s contention that the IRA’s requirement on drug manufacturers to pay Medicare rebates for price increases above inflation “may help reduce future growth in prescription drug spending.” But that’s not what the data show for the price of prescription drugs overall.
Background on the ASPE report
ASPE’s report evaluates total spending trends and further breaks out those trends by retail and non-retail drug spending. Retail generally refers to drugs purchased through a pharmacy and non-retail generally refers to drugs administered in a hospital or clinic. The report further breaks out spending trends for specialty drugs.
The report also evaluates total spending within these categories against the number of prescriptions filled. These two data points allow ASPE to identify spending per prescription. If the growth in spending per prescription drug exceeds the growth in total prescriptions, then this suggests prices are the main driver of higher spending. The primary data source for the report is the IQVIA National Sales Perspective data which, according to the report, represents 90 percent of the pharmaceutical market.
Report focuses on what drives spending increases for retail and non-retail drugs
Table 1 in the ASPE report shows a 12.5 percent increase in retail prescription drug spending and a 5.7 percent increase in the number of retail prescriptions. Looking then to spending growth per retail prescription, ASPE finds: “On average, there was a 7 percent increase in spending per prescription, which suggests that changes in utilization (i.e., a greater number of prescriptions being filled) were not the primary driver of increased retail drug spending.” Thus, for retail drugs, prices are the primary driver.
For non-retail drugs, ASPE finds the opposite is true. Table 1 shows a 25.1 percent increase in non-retail spending and a 19.2 percent increase in the number of non-retail prescriptions. ASPE’s data shows the growth in spending per non-retail prescription was much less than the growth in prescriptions. Thus, ASPE concludes: “On average, there was a 5 percent increase in the spending per prescription, meaning that the primary driver of increased non-retail prescription drug spending was greater utilization, rather than higher drug prices.”
ASPE data shows higher spending on all drugs is primarily driven by higher utilization
Oddly, this portion of the report does not provide a similar discussion on whether higher drug prices or utilization is responsible for the total increase in spending on all drugs. This is despite the fact that Table 1 breaks out data across retail, non-retail, and total. Instead, the report waits to mention it as an aside when discussing specialty drugs, stating: “The overall changes [in specialty drugs] resemble what was evident for all drugs, spending growth was largely due to higher prices per prescription, not increases in utilization” (emphasis added). The report’s conclusion then leads with same claim to identify the primary driver for higher prescription drug spending, claiming “This increase was driven by increases in spending per prescription, and less so by increases in the number of prescriptions.”
Yet, incredibly, page back from the report’s conclusion to Table 1 and the data shows the opposite. The data shows a 16.0 percent increase in spending on all drugs and a 10.9 percent increase in all prescriptions. Yet, on average, there was a 4.5 percent increase in spending per prescription. This is much lower than the growth in the number of all prescriptions. Using the same logical inferences ASPE used to show higher prices drive higher spending for retail drugs and higher utilization drives higher spending for non-retail drugs, this much smaller increase in spending per prescription strongly suggests increases in all drug spending was primarily driven by higher utilization.
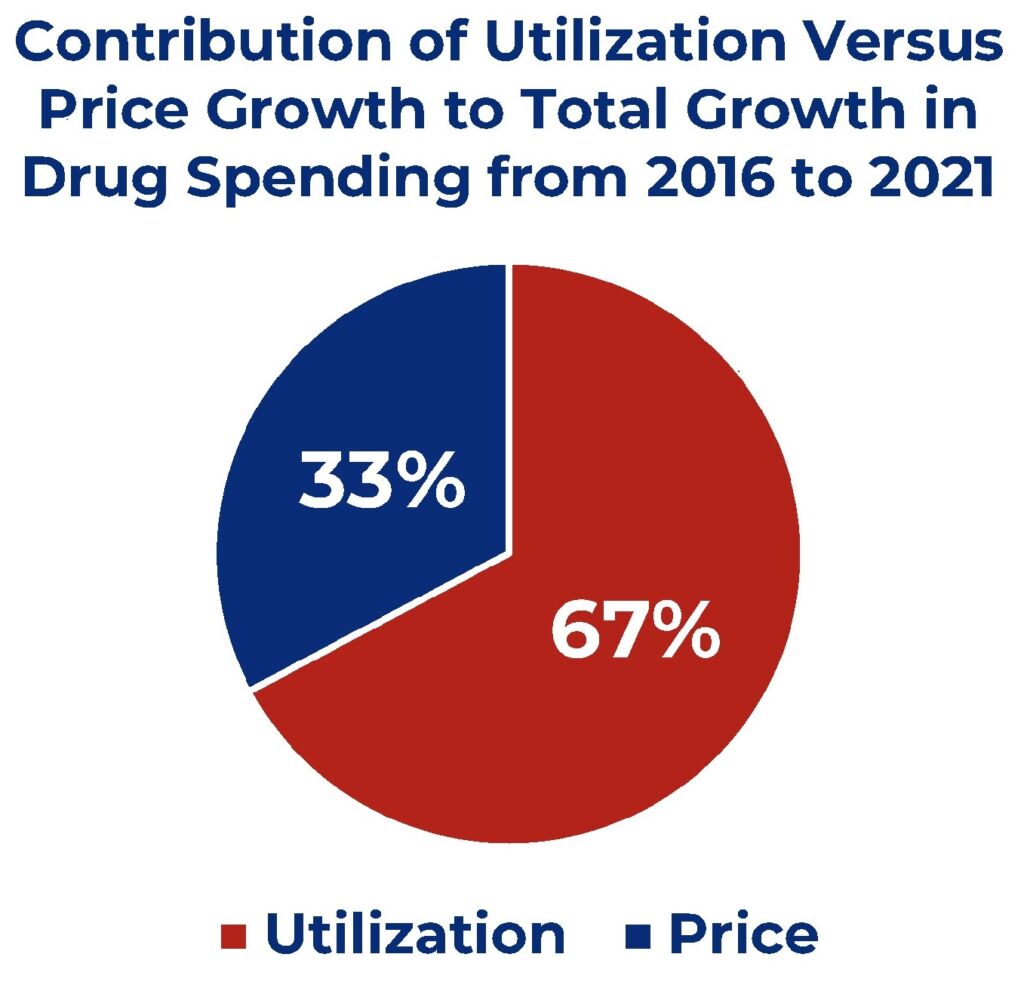
Using the data in the report, it’s possible to approximate the contribution of the growth in pricing versus the growth in utilization to the overall growth in drug spending. This simply requires multiplying the annual per prescription drug price growth rate by total spending from the previous year to isolate the portion of the spending increase due to higher drug prices from the previous year. Then subtract the portion due to higher drug prices from the total annual change in spending to establish the change in spending from utilization. Using this approach, the pie chart below shows 67 percent of the increase in spending on all drugs from 2016 to 2021 was driven by higher utilization.
Applying this approach to retail and non-retail drug spending shows ASPE correctly stated that growth in retail drug spending was largely driven by higher drug prices and growth in non-retail drug spending was largely driven by utilization. Higher prices account for 59 percent of the growth retail spending, while higher utilization accounts for 81 percent of the growth in non-retail drug spending. This much larger contribution of utilization to higher non-retail drug spending explains why the increase in spending on all drugs was driven more by higher utilization and less by higher prices.
Data shows only small increases in per prescription spending
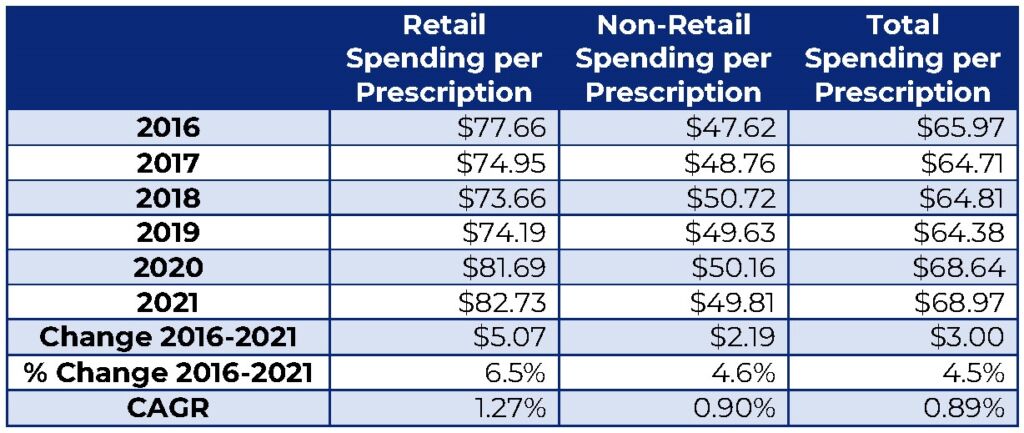
In addition to showing utilization is far more responsible for higher drug spending, the ASPE data shows only small annual increases in spending per prescription. The table below calculates the spending per prescription from Table 1 of the ASPE report. ASPE may have forgone this simple step because it would have revealed spending per prescription drug went up by just $3.00 for all drugs from 2016 to 2021. This comes to a compound annual growth rate (CAGR) of less than 1 percent. Growth in spending per retail drug is higher but is still only $5.07, representing 1.27 percent CAGR. These small increases do not fit the Biden administration’s narrative that rising drug prices are a major contributor to higher health care costs.
Prescription Drug Spending per Prescription
(in Inflation Adjusted Dollars), 2016-2021
ASPE’s data provides more evidence that IRA’s focus on drug prices was misplaced
This is all inflation adjusted and so it does represent a real increase in price. However, the price increase is much smaller by comparison to several other health sectors. The modest inflation adjusted increase supports National Health Expenditure (NHE) data that shows the recent growth in health spending is largely due to spending growth from hospital care and physician and clinician services.
American Experiment published a report analyzing the drug price controls in the IRA ahead of its passage. Our review of NHE data showed retail prescription drugs grew by 37 percent from 2010 to 2020. By comparison, hospital care spending grew by 57 percent and physician and clinical services spending grew by 58 percent. As a result of the lower growth rate, retail prescription drug spending dropped from 9.8 percent of NHE in 2010 to 8.4 percent in 2020.
NHE data also include a retail prescription drug price index that measures and isolates the annual change in drug prices. This data shows drug prices declined in 2018, 2019, and 2020, which is consistent with ASPE’s spending per prescription data until 2020.
This NHE data also allows a rough approximation of the proportion of the rise in NHE drug spending is attributable to prices. Our report estimates higher drug prices accounted for only 2.4 percent to the overall growth in health care costs from 2010 to 2020. Higher utilization accounted for 3.8 percent, meaning utilization was the primary driver for higher retail prescription drug spending. Notably, this NHE data suggests utilization accounted for 61 percent of the rise in retail drug spending. This is consistent with the ASPE data, but shows a longer-term trend in utilization being the main culprit for higher drug spending, not prices.
ASPE fails to put list prices in context
On top of misreporting the data, the report fails to properly put the data in context. The ASPE report acknowledges (the HHS press release does not) the spending data uses list prices before rebates. ASPE, however, fails to acknowledge how rebates have been rising faster than list prices, resulting in a lower inflation rate for net prices. From 2012 to 2017, research shows drug price inflation was 12 percent per year for list prices but only 3 percent for after rebate net prices.
Due to this finding, the study authors note that “analysts and economists working in public policy should be extremely cautious in drawing policy conclusions based on list prices alone.” Nonetheless, the Biden administration wants the public to draw conclusions on the benefits of the Inflation Reduction Act based on list prices alone. The second companion report, which did a slightly better job of putting the list price in context, also focused exclusively on the annual increase in list prices from 2016 to 2022.
Reporting list prices is still important as individual cost-sharing is often based on list prices. But net prices are what truly matters when trying to understand overall trends in prescription drug spending, which is what ASPE purports to study.
The strategy for pushing a false narrative
Even if the study was correct and higher drug prices were the primary driver of higher drug spending, this failure to put list prices in context exposes the strategy employed to push a false narrative.
- Step one, limit a study to data that supports your policy.
- Step two, allow the researchers to acknowledge the limitations of the data so they can sleep at night.
- Step three, minimize the acknowledgement in the report, preferably to a footnote or, even better, an endnote that requires page turning to find.
- Step four, issue a press release reporting the findings without acknowledging the limitations.
- Step five, enlist surrogates to propagate and reinforce the message.
Conclusion
It’s hard to understand how the reports’ authors ended up at their conclusion when the data clearly shows the opposite. Was it just an error that no one questioned because it conveniently fit the narrative? Or was it an intentional misrepresentation pulled in after the authors finished and sent the report up the chain for clearance and vetting? Regardless, this report shows the lack of seriousness the Biden administration brings to evaluating the impacts of their policies and the lengths they’ll go to spin data to advance a false narrative to support their agenda.